
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Thrombocytopenia
Similar to Thrombocytopenia (20)
More from Priya
More from Priya (20)
Recently uploaded
Recently uploaded (20)
Thrombocytopenia
- 2. INTRODUCTION The estimated prevalence of thrombocytopenia in MDS, defined as a platelet count of <100,000/mcL, ranges from 40% to 65%. A retrospective review of patients referred to the MD Anderson Cancer Center identified 1605 of 2410 (67%) patients with thrombocytopenia at referral. A normal human platelet count ranges from 150,000 to 450,000 platelets per microliter of blood. Values outside this range do not necessarily indicate disease. One common definition of thrombocytopenia requiring emergency treatment is a platelet count below 50,000 per microliter
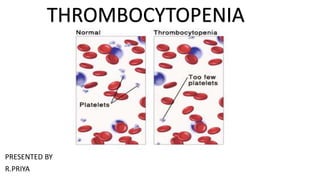
- 3. DEFINITION Thrombocytopenia is a condition characterized by abnormally low levels of platelets , also known as thrombocytes, in the blood. It is the most common coagulation disorder among intensive care patients and is seen in 20% of medical patients and a third of surgical patients.
- 4. CAUSES Decreased production of platelets Platelets are produced in your bone marrow. Factors that can decrease platelet production include: •Leukemia and other cancers •Some types of anemia •Viral infections, such as hepatitis C or HIV •Chemotherapy drugs and radiation therapy •Heavy alcohol consumption •Dehydration, Vitamin B12 or folic acid deficiency •Leukaemia, myelodysplastic syndrome, or aplastic anaemia •Decreased production of thrombo poietin by the liver in liver failure •Sepsis, systemic viral or bacterial infection •Leptospirosis •Hereditary syndromes[14] • ACTN1-related thrombocytopenia • A megakaryocytic thrombocytopenia with radio-ulnar synostosis • ANKRD26 related thrombocytopenia
- 5. CAUSES Increased breakdown of platelets Abnormally high rates of platelet destruction may be due to immune or nonimmune conditions, including:[15] •Immune thrombocytopenic purpura •Thrombotic thrombocytopenic purpura •Hemolytic–uremic syndrome •Disseminated intravascular coagulation •Paroxysmal nocturnal hemoglobinuria •Antiphospholipid syndrome •Systemic lupus erythematosus •Post-transfusion purpura •Neonatal alloimmune thrombocytopenia •Hypersplenism •Dengue fever •Gaucher's disease •Zika virus
- 6. CAUSES Some conditions can cause your body to use up or destroy platelets faster than they're produced, leading to a shortage of platelets in your bloodstream. Examples of such conditions include: •Pregnancy. Thrombocytopenia caused by pregnancy is usually mild and improves soon after childbirth. •Immune thrombocytopenia. Autoimmune diseases, such as lupus and rheumatoid arthritis, cause this type. The body's immune system mistakenly attacks and destroys platelets. If the exact cause of this condition isn't known, it's called idiopathic thrombocytopenic purpura. This type more often affects children. •Bacteria in the blood. Severe bacterial infections involving the blood (bacteremia) can destroy platelets. •Thrombotic thrombocytopenic purpura. This is a rare condition that occurs when small blood clots suddenly form throughout your body, using up large numbers of platelets. •Hemolytic uremic syndrome. This rare disorder causes a sharp drop in platelets, destruction of red blood cells and impairs kidney function. Medication-induced These medications can induce thrombocytopenia through direct myelosuppression: •Valproic acid •Methotrexate •Carboplatin •Interferon •Isotretinoin •Panobinostat •H2 blockers and proton-pump inhibitors •. Certain medications can reduce the number of platelets in your blood. Sometimes a drug confuses the immune system and causes it to destroy platelets. Examples include heparin, quinine, sulfa-containing antibiotics and anticonvulsants.
- 7. CAUSES Other causes •Lab error, possibly due to the anticoagulant EDTA in CBC specimen tubes;[citation needed] a citrated platelet count is a useful follow-up study •Snakebite •Niacin toxicity •Lyme disease •Thrombocytapheresis (also called plateletpheresis)[citation needed] •Niemann–Pick disease
- 9. SIGNS AND SYMPTOMS •red, purple, or brown bruises, which are called purpura •a rash with small red or purple dots called petechiae •nosebleeds •bleeding gums •bleeding from wounds that lasts for a prolonged period or doesn’t stop on its own •heavy menstrual bleeding •bleeding from the rectum •blood in your stool •blood in your urine In more serious cases, you may bleed internally. Symptoms of internal bleeding include: •blood in the urine •blood in the stool •bloody or very dark vomit
- 10. DIAGNOSTIC EVALUATION Blood tests To diagnose this condition, your doctor needs to do a complete blood count test. This test looks at the amount of blood cells in your blood. It’ll tell your doctor if your platelet count is lower than it should be. A typical platelet count will range between 150,000 and 450,000 platelets per mL blood. Your doctor may also wish to have your blood tested for platelet antibodies. These are proteins that destroy platelets. Platelet antibodies can be produced as a side effect to certain drugs, such as heparin, or for unknown reasons. Your doctor may also order blood-clotting tests, which includes partial thromboplastin time and prothrombin time. These tests simply require a sample of your blood. Certain chemicals will be added to the sample to determine how long it takes your blood to clot. Ultrasound If your doctor suspects that your spleen is enlarged, they may order an ultrasound. This test will use sound waves to make a picture of your spleen. It can help your doctor determine if your spleen is the proper size. Bone marrow aspiration and biopsy If your doctor suspects that there’s a problem in your bone marrow, they may order a bone marrow aspiration. During an aspiration, your doctor will use a needle to remove a small amount of bone marrow from one of your bones. A bone marrow biopsy may also be ordered. Your doctor will use a needle to take a sample of your core bone marrow, usually from the hipbone. It may be performed at the same time as a bone marrow aspiration. liver enzymes, kidney function, vitamin B12 levels, folic acid levels, erythrocyte sedimentation rate, and peripheral blood smear. If the cause for the low platelet count remains unclear, a bone marrow biopsy is usually recommended to differentiate cases of decreased platelet production from cases of peripheral platelet destruction.
- 11. MANAGEMENT •blood or platelet transfusions •changing medications that are causing a low platelet count •steroids •immune globulin •corticosteroids to block platelet antibodies •drugs that suppress your immune system •spleen removal surgery • Lithium carbonate or folate may also be used to stimulate platelet production in the bone marrow. • Discontinuation of heparin is critical in a case of heparin-induced thrombocytopenia (HIT). Beyond that, however, clinicians generally treat to avoid thrombosis. Treatment may include a direct thrombin inhibitor, such as lepirudin or argatroban. Other blood thinners sometimes used in this setting include bivalirudin and fondaparinux. Platelet transfusions are not routinely used to treat HIT because thrombosis, not bleeding, is the primary problem. Warfarin is not recommended until platelets have normalized.
- 12. THANK YOU